
Endometriosis is one of the most common and challenging gynaecological disorders, affecting 10-15% of women in the reproductive age. According to the original study by Dessole et al (2003) sonovaginography diagnosed rectovaginal endometriosis more accurately than did transvaginal ultrasonography, with a sensitivity and specificity of 90.6% and 85.7%, respectively, whereas the transvaginal ultrasonography has shown a sensitivity and specificity of 43.7% and 50%, respectively
“Please note it is essential to have a pelvic ultrasound done at POGU for your initial assessment of pelvic symptoms before proceeding to a Sonovaginography if necessary. This is because most patients with pelvic symptoms may not require this scan. If you have any queries, please contact our reception on 08 6162 1074.”
Sonovaginography is a detailed assessment of deep infiltrating endometriosis. According to the original study by Dessole et al (2003) sonovaginography diagnosed rectovaginal endometriosis more accurately than did transvaginal ultrasonography, with a sensitivity and specificity of 90.6% and 85.7%, respectively, whereas the transvaginal ultrasonography has shown a sensitivity and specificity of 43.7% and 50%, respectively.
What is endometriosis?
Endometriosis is one of the most common and challenging gynaecological disorders, affecting 10-15% of women in the reproductive age group. Endometriosis is a condition in which bits of the tissue similar to the lining of the uterus (endometrium) grow in other parts of the body. Like the uterine lining, this tissue builds up and sheds in response to monthly hormonal cycles. However, there is no natural outlet for the blood discarded from these implants. Instead, it falls onto surrounding organs, causing swelling and inflammation. This repeated irritation leads to the development of scar tissue and adhesions (stickiness) between pelvic organs in the area of the endometrial implants. Common symptoms include pelvic pain, pain with periods, pain with sex, bowel pain during periods, and infertility.
What is the role of ultrasound in the diagnosis of endometriosis?
Endometriosis is one of the most common and challenging gynaecological disorders, affecting 10-15% of women in the reproductive age group. Endometriosis is a condition in which bits of the tissue similar to the lining of the uterus (endometrium) grow in other parts of the body. Like the uterine lining, this tissue builds up and sheds in response to monthly hormonal cycles. However, there is no natural outlet for the blood discarded from these implants. Instead, it falls onto surrounding organs, causing swelling and inflammation. This repeated irritation leads to the development of scar tissue and adhesions (stickiness) between pelvic organs in the area of the endometrial implants. Common symptoms include pelvic pain, pain with periods, pain with sex, bowel pain during periods, and infertility.
The majority of women with endometriosis have superficial endometriosis and these lesions are too small to be seen on routine pelvic ultrasound. The gold standard for diagnosing this form of endometriosis is laparoscopy. A sub-group of women however will have more severe form of the disease, which is called as ‘deep infiltrating endometriosis’. Deep infiltrating endometriosis causes usually more destruction of the normal anatomy. Because lesions of endometriosis infiltrate into ligaments, bowel and bladder, adhesions can occur between organs such as the bowel and the uterus or the uterus and the ovaries.


Treatment of endometriosis is difficult, particularly in case of DIE
Physical examination has a very limited ability to diagnose and quantify deep infiltrating endometriosis. Recent improvements in ultrasound techniques have led to early diagnosis of deep infiltrating endometriosis on an expert ultrasound assessment. This has led to earlier diagnosis, reduction of surgical risk, possibility to use medical treatment prior to surgery, and improvement of pre-operative planning if surgery is required
Deep infiltrating endometriosis constitutes a major concern for the gynaecologist in view of the greater severity of symptoms associated with this form of the disease and the complexity of the treatment involved. Preoperative staging of DIE is crucial for planning appropriate surgical intervention and for planning the multi disciplinary team who may be involved in the care.
How is the scan done for deep infiltrating endometriosis?
The best method to assess the potential areas of endometriosis using ultrasound involves preparation of the bowel to reduce the impact of faecal matter and gas in the colon and rectum prior to having the ultrasound. To prepare the bowel, you will need to take:
- Low residue diet x 1 day
- Two tablets of Dulcolax at night times for 3 days before your scan (This is a mild laxative)
- A fleet enema administered by yourself (This enema is expected to have an effect within 10- 15 minutes)


More detailed information on bowel preparation will be given to you once an appointment is made for your scan.
You will be asked to empty your bladder and the assessment will be done by the transvaginal approach with a slender ultrasound probe being passed into the vagina. Sterile ultrasound gel is also inserted into the top of your vagina to aid views of the vaginal wall. The whole procedure may take up to about 30 minutes depending on the degree of difficulty of assessing your pelvis.
Each ultrasound examination is interpreted and documented in real time by the specialist. Routine analysis of the uterus and ovaries are done initially. A detailed assessment of the peritoneal surface covering the vesicouterine pouch, the pouch of Douglas, the bowel (rectum, sigmoid colon up to 30cm from the anal verge), the uterosacral ligaments, posterior vaginal fornix, and the rectovaginal septum is done for mapping the extent and severity of endometriosis lesions. The bowel preparation allows loops of the bowel to be examined in detail, a procedure that would be impossible if air or fecal residues were degrading the ultrasound beam.
A large ovarian endometrioma
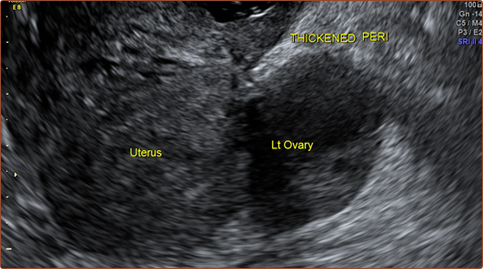
Retroflexed fixed uterus with adherent ovary and thickening of tissues on top of the vagina.
![]()
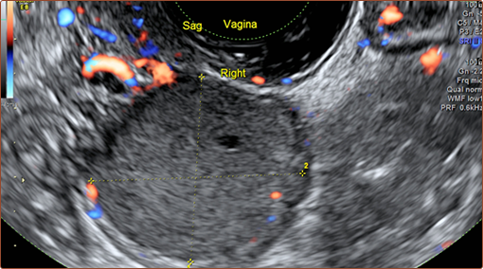
Transverse image of right ovary with multiple endometriomas, which is adherent to the vaginal endometriosis nodule and bowel loops. Cervix is seen deviated to right and is also rotated.
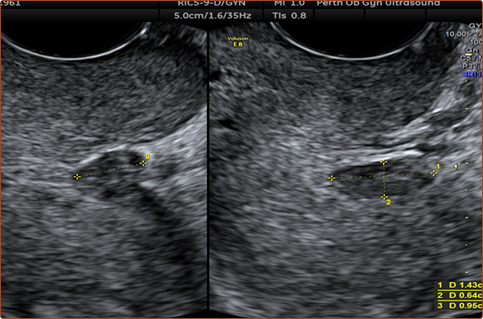
Bilateral uterosacral nodules
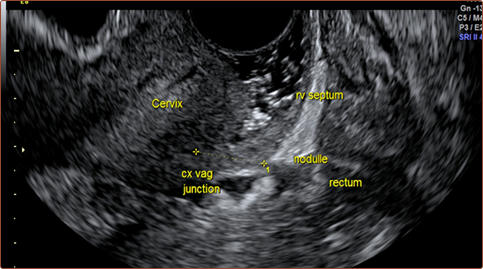
Rectovaginal septum nodule
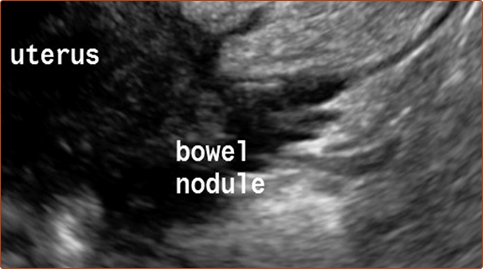
Large bowel nodule seen adherent to the fundus of the uterus. Uterus was found to be retroflexed and in affixed position
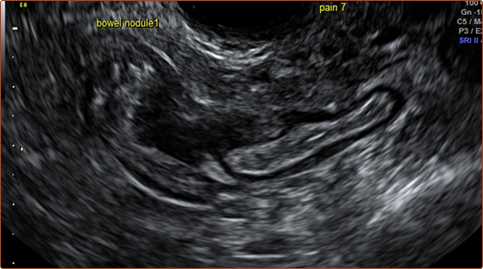
A bowel nodule in a free lying loop of bowel

Complex lesions in a patient with previous hysterectomy for endometriosis
Does the scanning cause pain?
The examination may be associated with more discomfort or pain than usual, due to extra pressure on the bowel. If you are concerned about pain, you may like to consider taking simple painkillers shortly before you leave home- e.g. Panadol, Panadeine or Nurofen. If necessary, you can also take simple painkillers following your scan during the day.
Is there an ideal time for the ultrasound examination?
It is most convenient if your scan is scheduled in the 2 weeks leading up to your expected period, preferably the 3rd week of your menstrual cycle. This is most suitable as patients with endometriosis have least amount of pelvic pain during this particular time period. Although a scan can be performed during a period, this is likely to be a time of increased pain for women with endometriosis, and we would therefore recommend avoiding this if possible. However, please note that it is not always possible to schedule medical appointments at the most ideal time
What is the set up of our service?
In our practice this new procedure for assessing severe endometriosis is currently provided by Dr. Thottungal who established this service in Western Australia in 2011. Women undergoing this examination will receive the highest quality expert opinion on their ultrasound to help guide their management. Women can also expect that at the completion of scan, the findings will be sympathetically discussed with them. The information obtained from the scan will be given to your referring doctor for discussion with you at your next appointment.